School is back and with it comes the now-annual debate over whether kids should be obligated to wear masks so long as Covid19 continues circulating. Here are 19 reasons they shouldn't:
Without clear, provable evidence that masks curtail Covid, commonsense suggests schools should err on the side of caution and minimize disruption to children's lives.
Since Covid emerged, there has yet to be a single study showing masks are efficacious in slowing the spread of Covid. The CDC itself has admitted as much: "CDC is not aware of any randomized controlled trials that show that masks or double masks or cloth face coverings are effective against COVID-19."
The lack of studies showing masks are useful is unsurprising given what we now know about the virus — namely that it’s an aerosolized pathogen whose particle size typically ranges from 0.06 microns to .14 microns (roughly the same size as cigarette smoke); even the best masks on the market, the N95, only filters down to 0.3 microns. So, N95 masks block few, if any, virus particles.
An adviser to the UK’s Scientific Advisory Group for Emergencies, Dr. Colin Axon, says masks have gaps 5,000 times larger than Covid particles. “A Covid viral particle is around 100 nanometres, material gaps in blue surgical masks are up to 1,000 times that size, cloth mask gaps can be 500,000 times the size,” he said. “The small sizes are not easily understood but an imperfect analogy would be to imagine marbles fired at builders’ scaffolding, some might hit a pole and rebound, but obviously most will fly through.”
(If anyone wants to test this themselves, take a drag of a cigarette and then exhale through a mask; the smoke represents Covid; if it escapes, the mask hasn’t worked … or you can watch this if you don’t care to smoke.)
Tweet #1398023020808134656
While there’s yet to be a study showing masks help curtail Covid, there are now more than a dozen showing they explicitly don’t work [links via Swiss Policy Research]:
A May 2020 meta-study on pandemic influenza published by the CDC found that face masks had no effect, neither as personal protective equipment nor as a source control. (Source)
Danish randomized controlled trial with 6,000 participants, published in the Annals of Internal Medicine in November 2020, found no statistically significant effect of high-quality medical face masks against SARS-CoV-2 infection in a community setting. (Source)
A large randomized controlled trial with close to 8,000 participants, published in October 2020 in PLOS One, found that face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.” (Source)
A February 2021 review by the European CDC found no high-quality evidence in favor of face masks and recommended their use only based on the ‘precautionary principle’. (Source)
A July 2020 review by the Oxford Centre for Evidence-Based Medicine found that there is no evidence for the effectiveness of face masks against virus infection or transmission. (Source)
A November 2020 Cochrane review found that face masks did not reduce influenza-like illness (ILI) cases, neither in the general population nor in health care workers. (Source)
A July 2021 experimental study published by the American Institute of Physics found that face masks reduced indoor aerosols by at most 12%, not enough to prevent infections. (Source)
An April 2020 review by two U.S. professors in respiratory and infectious disease from the University of Illinois concluded that face masks have no effect in everyday life, neither as self-protection nor to protect third parties (so-called source control). (Source)
An August 2021 study published in the Int. Research Journal of Public Health found “no association between mask mandates or use and reduced COVID-19 spread in U.S. states.” (Source)
An article in the New England Journal of Medicine from May 2020 came to the conclusion that face masks offer little to no protection in everyday life. (Source)
A 2015 study in the British Medical Journal BMJ Open found that cloth masks were penetrated by 97% of particles and may increase infection risk by retaining moisture or repeated use. (Source)
An August 2020 review by a German professor in virology, epidemiology and hygiene found that there is no evidence for the effectiveness of face masks and that the improper daily use of masks by the public may in fact lead to an increase in infections. (Source)
Several case studies have found children don’t spread Covid in schools. Before vaccines were widely available, A North Carolina study found not a single case of student-to-teacher transmission among more than 90,000 students.
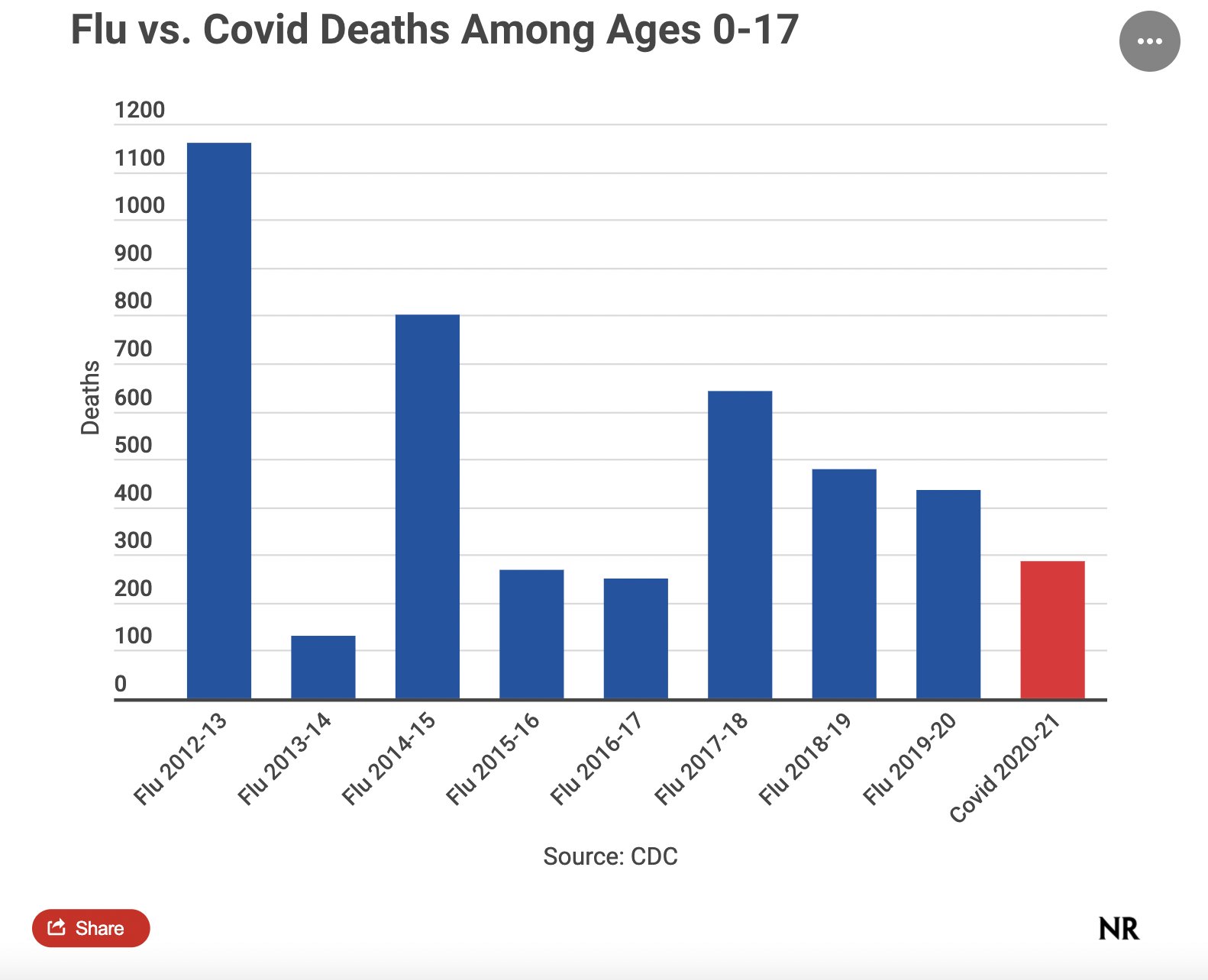
Less than 300 children have died from issues related to Covid — far fewer than die from the flu in an average year. Schools have never required masks to stop the spread of various flu strains, and there’s no reason kids should be treated more harshly for a virus that’s less dangerous. [Chart via Phil Klein]
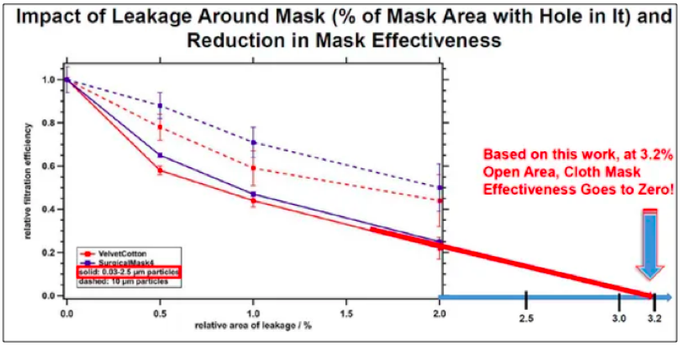
When worn on adults, every mask — even expensive surgical and N95 masks — have gaps where air escapes. Typical cloth masks have a gap of ~3.2 percent. As you can see in the chart below, the supposed effectiveness of masks diminishes to zero with a 3.2 percent threshold. When children wear masks, the gap is always invariably larger. [Chart via Emily Burns]
Mandated masking is associated with decreased socialization. A study of Hong Kong preschoolers during the 2003 SARS outbreak found that masked children decreased their socializing among peers; students additionally felt discomfort wearing masks and struggled reading facial expressions of their peers and teachers.
The WHO recommends children 6 and under not to wear masks and urges caution with those 12 and under.
While masks haven’t proven effective against Covid, a study found that masking children can cause hypercapnia, a dangerous buildup of carbon dioxide in your bloodstream.
Hypercapnia is potentially why schools in Tianjin and Shanghai, China, canceled physical examinations after two masked 14-year-old boys collapsed and died while running one-mile during gym class.
Children forced to wear masks sometimes suffer breathing difficulties, for which they compensate by mouth breathing. “Chronic and prolonged mouth breathing can alter facial development,” Drs. Marty Makary and H. Cody Meissner recently wrote. “It is well-documented that children who mouth-breathe because adenoids block their nasal airways can develop a mouth deformity and elongated face.”
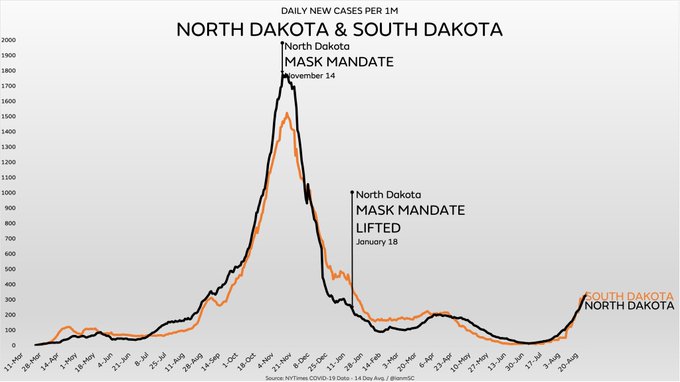
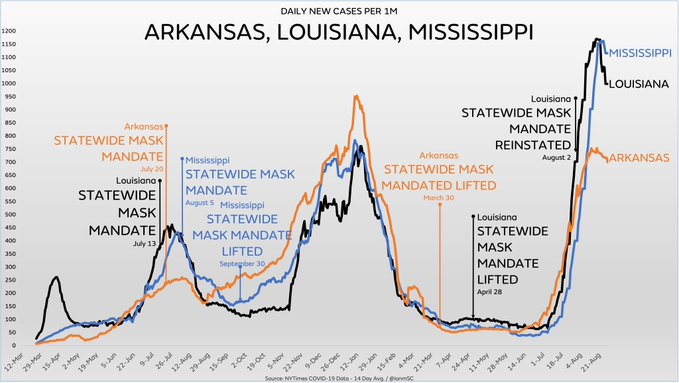
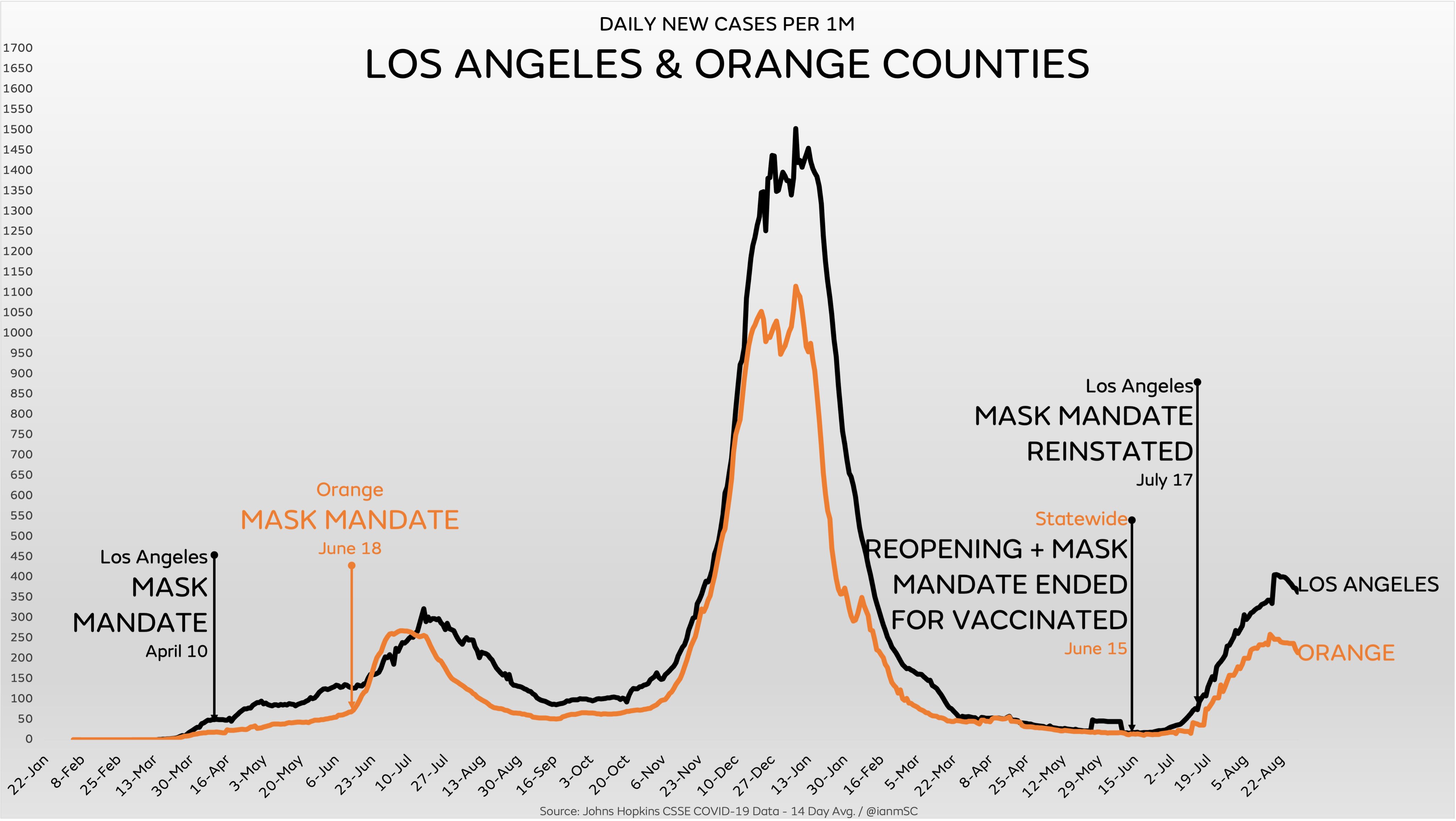
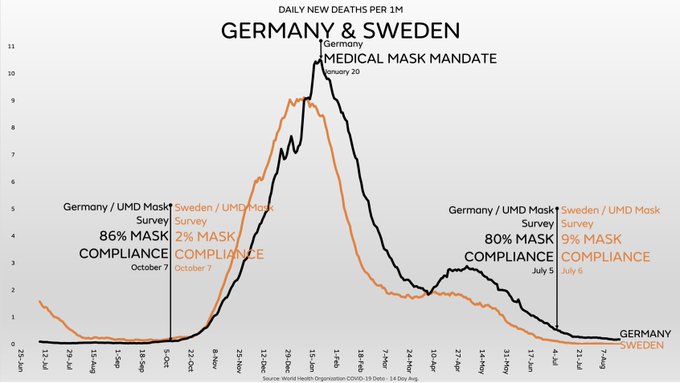
In the United States, states without mask mandates have similar case curves as states with mask mandates and if anything, tend to actually outperform states with greater restrictions. The same can also be seen when comparing a European country with universal N95 masking (Germany) vs. a European country without a mask mandate and little mask usage (Sweden). [Graphs via Ian Miller]
A meta analysis of American schools in 2020 shows that schools with the strictest Covid protocols actually produced worse outcomes than those with more relaxed protocols.
Mask mandates can be particularly problematic for teenagers. “Masks can cause severe acne and other skin problems. The discomfort of a mask distracts some children from learning. By increasing airway resistance during exhalation, masks can lead to increased levels of carbon dioxide in the blood,” Drs. Makary and Meissner wrote.
Pediatricians report masking & forced social isolation is retarding children’s social development. “We’ve seen some language delays and more social anxiety. The inability of a child to leave their parent and go play with other children,” said System Chair of Pediatrics at Allegheny Health Network, Dr. Joseph Aracri.
Another study, this one from the Warren Alpert Medical School at Brown University, found that masks are impairing early childhood development:
“Leveraging a large on-going longitudinal study of child neurodevelopment, we examined general childhood cognitive scores in 2020 and 2021 vs. the preceding decade, 2011-2019. We find that children born during the pandemic have significantly reduced verbal, motor, and overall cognitive performance compared to children born pre-pandemic. Moreover, we find that males and children in lower socioeconomic families have been most affected.”
An expert in childhood trauma at Columbia University recently wrote that mask mandates are inflicting slow-motion trauma upon children that can take years to fully manifest:
More studies should be conducted on just how traumas from Covid-19 restrictions in schools are associated with the long-term health and well-being of American children, but research on Post-Traumatic Stress Syndrome has illuminated that “stress and fear, in response to actual or possible threat, enhances the possibility of forming trauma-related memories.” Every year of a child’s early life lays the foundation for their adulthood and insecure foundations do, in fact, crumble. According to Maslow’s Hierarchy of Needs, children without assurance of their personal security (e.g. social anxiety from masks and social distancing) are often incapable of making healthy social connections and may have difficulty building intimate relationships in their lives. Neurological research demonstrates that kids who experience this kind of fear and trauma at a young age undergo structural and functional restructuring of their brain’s prefrontal cortex, resulting in emotional and cognitive processing problems. This trauma is especially concerning for children growing up in poverty who often have the compounding effect of other trauma at home or in their community.
Florida scientists tested masks worn by school children and found they had accumulated up a number of dangerous contaminants. “Although the test is capable of detecting viruses, including SARS-CoV-2, only one virus was found on one mask (alcelaphine herpesvirus),” the science site, Rational Ground, reported. The contaminants discovered on the children’s masks included:
Streptococcus pneumoniae (pneumonia)
Mycobacterium tuberculosis (tuberculosis)
Neisseria meningitidis (meningitis, sepsis)
Acanthamoeba polyphaga (keratitis and granulomatous amebic encephalitis)
Acinetobacter baumanni (pneumonia, blood stream infections, meningitis, UTIs—resistant to antibiotics)
Escherichia coli (food poisoning)
Borrelia burgdorferi (causes Lyme disease)
Corynebacterium diphtheriae (diphtheria)
Legionella pneumophila (Legionnaires’ disease)
Staphylococcus pyogenes serotype M3 (severe infections — high morbidity rates)
Staphylococcus aureus (meningitis, sepsis)
”Half of the masks were contaminated with one or more strains of pneumonia-causing bacteria,” journalist Jennifer Cabrera reported. “One-third were contaminated with one or more strains of meningitis-causing bacteria. One-third were contaminated with dangerous, antibiotic-resistant bacterial pathogens. In addition, less dangerous pathogens were identified, including pathogens that can cause fever, ulcers, acne, yeast infections, strep throat, periodontal disease, Rocky Mountain Spotted Fever, and more.”